
The mixed episode is probably the most terrifying episode of bipolar disorder. Some will tell you that if they put themselves in the gravest danger, the mixed episode was likely the precursor. Less than half of people with bipolar disorder will experience such an episode at least once in their lifetime. The accounts and testimonies of those affected are chilling. Long considered an episode specific to bipolar type I, it is now known that all types are concerned.
📋 TL;DR : Mixed episode in short
- 🌪️ Mixed episode = depression + mania/hypomania coexisting.
- ⚡ Energy + despair = a high-risk combination.
- 😴 Insomnia, agitation, suicidal thoughts, extreme irritability.
- 🌀 More dangerous than mania or depression alone.
- 🏥 Often requires rapid hospitalization.
The mixed episode actually combines the chaos of a manic episode (or the euphoria of a hypomanic episode) with the symptoms of a depressive episode. While this may seem nonsensical to the untrained eye, it is a reality for many patients living with bipolar disorder. One study showed that 40% of bipolar patients will experience such an episode once in their lifetime. Although it is not limited to manic episodes, it is nevertheless less frequently observed during hypomanic episodes. For the sake of simplicity, I will refer to “mixed episodes” in this blog, even though the DSM-5 no longer mentions this type of episode.
The DSM definition
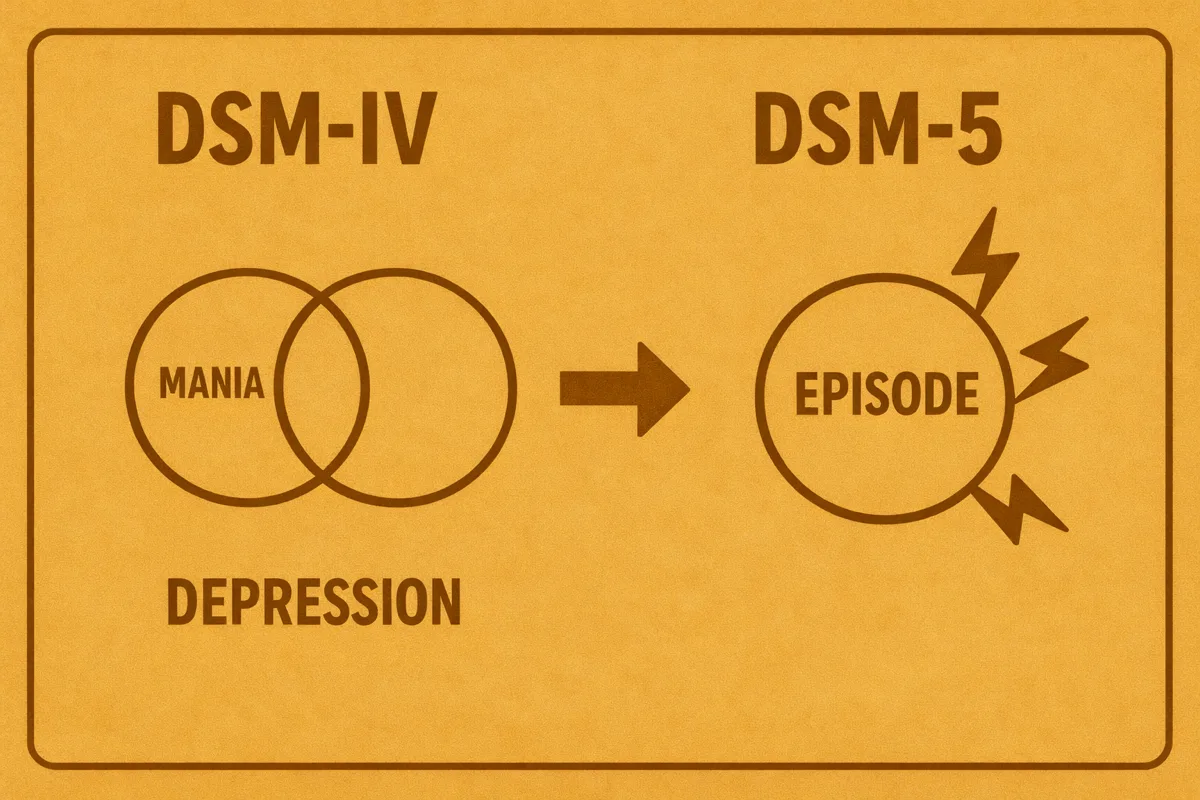
In the DSM-IV
In the DSM-IV and its revised version published in 2000, a mixed episode was described as requiring that all the minimum diagnostic criteria for (hypo)mania and those for depression be met simultaneously. For example, it could be defined by a euphoric, disinhibited, and logorrheic patient, but also presenting constant sadness, guilt, loss of interest, and suicidal thoughts.
In the DSM-5, currently
After its publication in 2013, the DSM-5 revisited this terminology. It now refers to “mixed features” that can be associated with hypomanic and manic episodes, as well as with depression, whether unipolar or bipolar. It is therefore important to note that even a non-bipolar patient with major depression may exhibit (hypo)manic symptoms.
Prevalence is nevertheless significantly higher among people with bipolar disorder, particularly in patients with bipolar disorder type I at around 20% and type II at around 5%, according to a study.
Unipolar patients may therefore present mixed features without exhibiting enough diagnostic symptoms of bipolar disorder. As a brief aside, it should be noted that these patients usually do not respond as well to antidepressants (which are otherwise very effective in major depression) and require a pharmacological approach closer to that used in bipolar disorder (mood stabilizers). Some researchers increasingly put forward the idea of a bipolar spectrum that would influence so-called unipolar individuals.
A document from the American Psychiatric Association (responsible for the DSM-5) explains how the DSM-IV criteria were too restrictive and rarely met by patients. The DSM-5 aims to encompass a broader range of patients.
The DSM-5 definition
In the DSM-5, to qualify an episode with mixed features, there are three criteria:
- Present a full episode (with its own diagnostic criteria) accompanied by at least 3 symptoms from the opposite pole.
- Symptoms present almost every day, for most of the duration of the current episode.
- Symptoms observable by others and representing a notable change from usual functioning.
It also distinguishes criteria attributable to the underlying pathology (for example: agitation, irritability present in both (hypo)mania and depression).
This means that the DSM-5 led to an increase in the prevalence of mixed episodes, as only 3 opposite criteria are now required. It should also be noted that the main pole is the one that is diagnosed, and that mixed features may not be constant. They only need to represent the majority of the episode. Manifestations are now considered specific depending on the dominant pole.
Its manifestations
Mixed features may vary depending on the nature of the episode.
Hypomania/mania with mixed features, the most common
- Dominant pole: Elation or irritability, inflated self-esteem, pressured speech, hyperactivity, reduced need for sleep, risk-taking
- Opposite pole:
- Depressive mood at times
- Loss of interest or pleasure
- Reduced sleep with experienced fatigue
- Guilt, low self-worth
- Thoughts of death
- Subjective experience: The patient feels both euphoric and desperate, shifting from laughter to tears.
- Risks: Very unstable and aggressive episodes, increased impulsivity, behavioral unpredictability.
- Prevalence: More often observed in type I.
Depression with mixed features
- Dominant pole: Sadness, anhedonia, psychomotor slowing, fatigue, guilt, thoughts of death.
- Opposite pole:
- Pressured speech despite sadness
- Flight of ideas or tachypsychia
- Agitation
- Reduced sleep without fatigue
- Impulsivity
- Subjective experience: The patient feels desperate but at the same time “wired,” internally agitated, unable to rest.
- Risk: Very high suicide risk due to collapsed mood combined with increased energy.
- Prevalence: More often observed in type II.
My testimony of a mixed episode
During a mixed episode, I experience an inner chaos even worse than manic chaos. Worse in the sense that it disorganizes my thoughts, annihilates any hope of getting better, and directs my thinking toward a single, ultimate goal: becoming an infernal machine of destruction, around me and toward myself. Suicide becomes the only conceivable solution to resolve a problem that is totally incomprehensible to me. I go through all emotions at once and am completely powerless in the face of an episode that is clearly more powerful than the feeling of invincibility that inhabits me.
I will explore my experience in greater depth with a detailed testimony in a future article.
Its hallmark symptoms
Mixed episodes differ from (hypo)manic episodes and depressive episodes by various criteria typically observed in those affected.
😡 Irritability and explosive anger
After the euphoric mood of mania, in a mixed episode there is instead marked irritability and a heightened expression of anger. Where mania produces an electric sensation running through the body, the mixed episode more often induces a very unpleasant electric tension. The person is “on edge” all the time.
💀 Very high suicide risk
Suicidal thoughts are a diagnostic criterion of depression in bipolar disorder. Most often, the patient does not have enough energy to act on them. The mixed episode often brings strong energy from the hypomanic or manic pole, making the person much more likely to have enough energy to act. These episodes frightened me for this reason; they are the closest I have come to the idea of having nearly ended my life.
If you yourself are in danger, consider visiting the Help and support page where you will find hotlines and online help.
🌙 Insomnia and tachypsychia
During a mixed episode, the person is often unable to sleep or simply does not want to. They remain very energetic, notably because of tachypsychia. Ideas race and prevent any hope of rest. All of these ideas are dark and guilt-laden, often pushing the patient to ruminate instead of sleeping. It is described as hell: impossible to sleep, yet impossible to stop thinking.
🚶♂️ Psychomotor agitation
As in a manic episode, the patient is subject to strong psychomotor agitation that drives them to walk, even wander, without purpose. The body seems to move on its own, even when the person tries to rest. During a manic episode, when I try to sleep, my body moves on its own incessantly. When I am awake, I pace around my apartment waiting for time to pass.
🎢 Emotional roller coaster
While a manic episode intensifies emotions, a mixed episode induces marked emotional lability: the person can shift from euphoria to tears to joy very quickly, sometimes within a few minutes. The sensation is terrifying.
Autism and the mixed episode
This section will be short. The reason is simple: I simply do not know how this episode interacts with my autism. Each time I experienced it, I was too busy enduring the pain and entering survival mode to be able to pay attention to it. I only know that all my thoughts revolved around survival instinct and suicide as the only solution, that I no longer paid attention to my routines or rituals. The mixed episode leaves me in a state where I lose my capacity for observation and perspective.
A study suggests that autistic people with bipolar disorder are more prone to mixed episodes than the norm. This is confirmed by another study on mixed depressive states experienced by autistic individuals.
Treatment
The Advanced Psychiatry Associates emphasizes that, like a manic phase, a mixed episode is a medical emergency—probably an even more critical one. The episode is very severe and, regardless of its intensity, must be treated as quickly as possible, often requiring hospitalization. My first mixed episode ended when I agreed to resume my treatment, to which my psychiatrist added a high-dose antipsychotic. Antipsychotics work relatively quickly, and within a few days, I was already feeling better.

Note to bipolar readers: even in the depths of despair, when everything seems doomed to fail, it is important never to stop your treatment without medical advice. The risk is worsening the episode.
📋 TL;DR : Keep in mind
- Combines depressive symptoms (dark thoughts, guilt, sadness) with (hypo)manic symptoms (energy, agitation, pressured speech).
- Affects about 40% of people with bipolar disorder over their lifetime, more frequent in type I.
- In the DSM-5, this is referred to as “mixed features”: a full episode plus at least 3 symptoms from the opposite pole.
- Typical symptoms: explosive irritability, insomnia, tachypsychia (rapid, dark thoughts), psychomotor agitation, emotional roller coasters.
- Major risk: higher dangerousness than depression or mania alone, particularly increased suicide risk.
- Subjective experience: inner chaos, constant tension, loss of usual reference points.
- Management: psychiatric emergency often requiring hospitalization and appropriate medication.