In the collective imagination, an autistic person is someone who is calm, withdrawn, asocial and, for some, exceptionally good at mathematics. Television stereotypes do little to dispel these ideas. Many still have Rain Man in mind, with its autistic character stopping in the middle of the road when the light turns red. The reality, however, is very different. Autism is a spectrum and expresses itself differently in each individual. Following my series of articles describing autism, it is time to produce a summary article addressing it in its full complexity.
📋 TL;DR: Autism in short
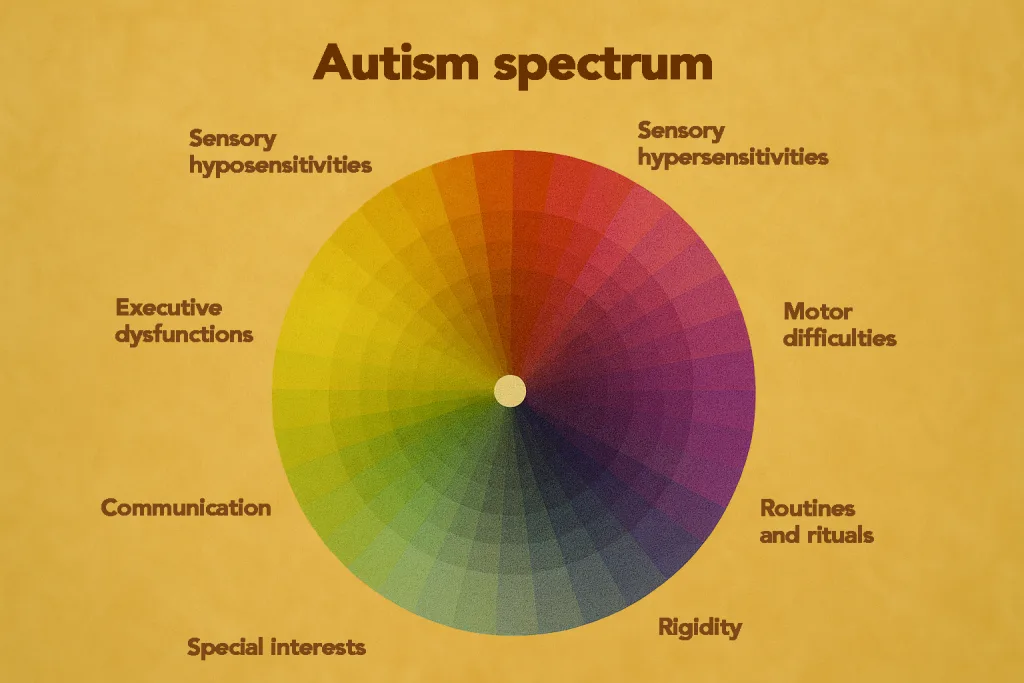
- Autism = spectrum: it manifests differently in each person, far from clichés (Rain Man, asocial genius).
- Difficult diagnosis: significant delays in France, persistent medical stereotypes, long and exhausting pathway.
- Compensation: many autistic people mask their difficulties, especially women and those with high IQ.
- Lived experience: assessments (ADI-R, IQ, ADHD, social cognition) are demanding and can trigger shutdowns or burnout.
Autism is a neurodevelopmental condition that long remained stereotyped, even among professionals. This greatly complicates diagnosis, which is significantly delayed in France. “But you make eye contact,” “You understand when I speak to you,” “You have friends/a boyfriend/a girlfriend”—these are all comments that concerned individuals may hear when seeking an assessment. Yet it has been known for years that many autistic people can mask so effectively that they may appear typical and only “atypical.” In psychiatry, this is referred to as compensating for one’s difficulties.
The person creates and adopts compensatory strategies to function as well as possible in a world that was not designed for them. These strategies are observed especially in women and, in some cases, in people with high IQ. I use the term “women” here because they are the most studied and most affected by diagnostic bias. However, these remarks also apply to other people assigned female at birth or perceived as feminine.
To illustrate these diagnostic delays, clinicians at the hospital where I was assessed explained that autism research and clinical recognition have historically progressed at different speeds across countries. In France in particular, adult autism—especially in people without intellectual disability—has long been under-recognized, which contributes to frequent late diagnoses.
The diagnostic pathway
Its stages
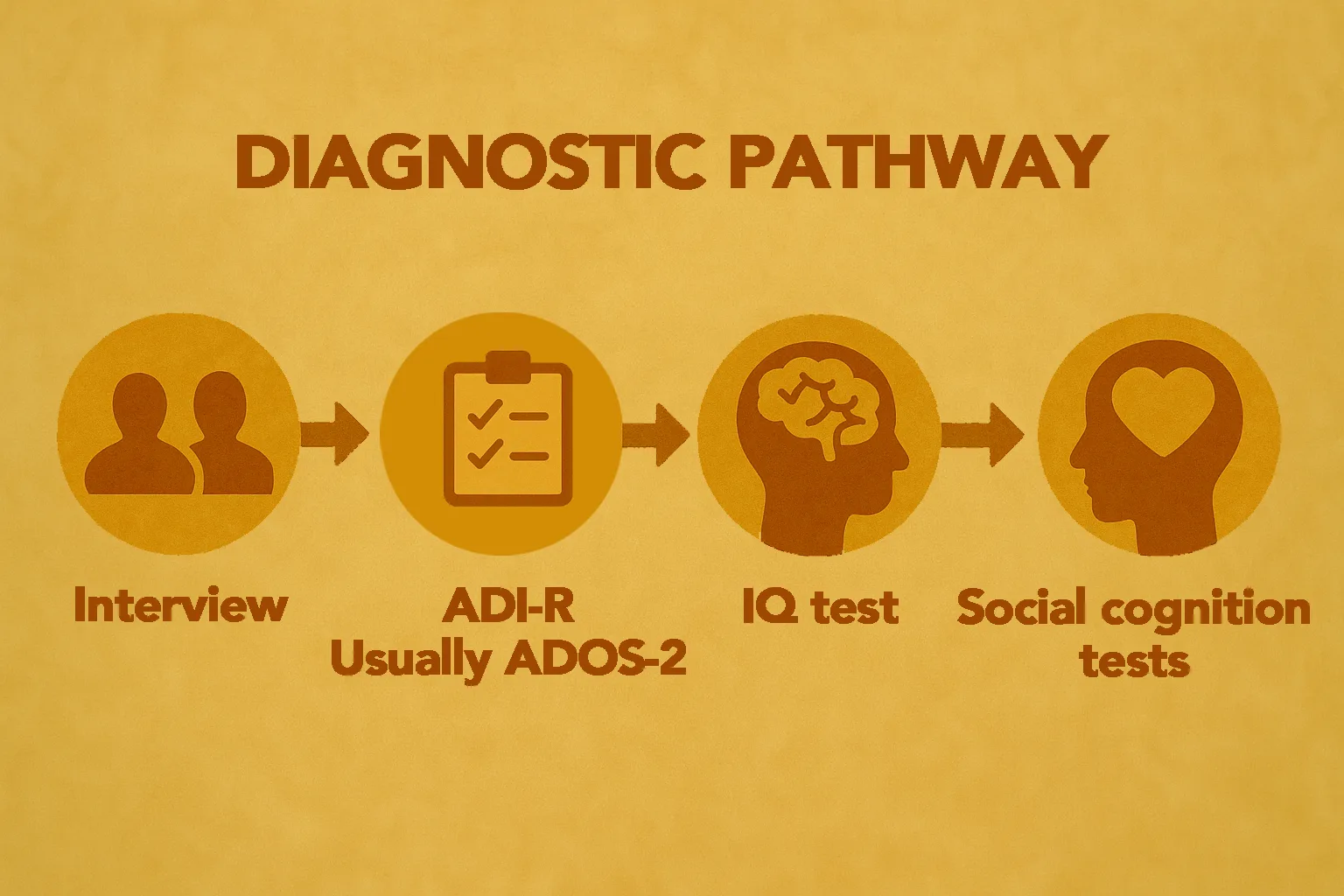
In any case, the diagnostic journey is often a harsh, long, and exhausting process for autistic people. In addition to frequently calling their entire life experience into question, they are subjected to batteries of tests that can be extremely demanding. Mine took place over five half-days: the initial interview to assess whether it was worthwhile to continue testing, the anamnesis, the ADI-R (a long early-childhood questionnaire designed to identify whether autistic traits were present early on), a three-hour IQ test, tests related to ADHD and executive functions, and social cognition tests. These last three triggered massive shutdowns—autistic crises—at the end of the day.
An exhausting process
I was in the middle of autistic burnout, and the tests were so thorough and tedious that they were enough to overload me and trigger the crisis. This is in fact often reported by patients: the need for a legitimate diagnosis requires going through this heavy process, but it is precisely so demanding that many feel like giving up (and sometimes do abandon midway through). I felt like quitting after each crisis, but my need to have an answer was a powerful driver that pushed me to the end.
It is paradoxical: we diagnose people who often fatigue more easily than average using tests that are themselves extremely exhausting. It is worth noting that autistic people generally have a lower tolerance threshold for fatigue than average. Tools (such as the spoon theory) also exist to help those concerned identify and manage their fatigue.
What is autism?
Autism is a neurodevelopmental condition. This means it manifests in utero, before birth. In other words, the brain develops atypically prior to birth. This development is so different (and unique to each autistic person) that we speak of neurodivergence. Every autistic person is unique, but there is a well-defined list of traits.
The DSM-5 definition
Autism is defined by specific criteria in the DSM-5 (the Diagnostic and Statistical Manual of Mental Disorders):
- Communication and social interaction (all must be present):
- Difficulties with reciprocity (e.g., understanding or initiating exchanges)
- Difficulties with body language, eye contact, gestures
- Difficulties creating or maintaining relationships
- Behaviors and interests (at least two must be present):
- Repetitive behaviors or speech (stimming)
- Rigid routines, need for sameness
- Highly intense specific interests
- Atypical sensitivity to sounds, lights, textures, etc. (sensory hyposensitivities and/or hypersensitivities)
- These differences must be present from childhood and have a significant impact on daily life (notable impairment).
Some scientific explanations
Studies have shown that brain structure develops differently from the norm. This may be explained by local hyperconnectivity (denser networks in certain regions) and long-range hypoconnectivity (less efficient connections between some distant regions), as suggested by this study (Molecular Autism, 2024, Contracted Functional Connectivity in Autism). Embrace Autism has also published a popularized article on this topic.
This local hyperconnectivity manifests as an atypical way of processing information. It favors attention to detail, regularities, and selective visual memory. Long-range hypoconnectivity translates into greater difficulty integrating information globally.
On the sensory level, the autistic brain also differs in the excitability of certain regions involved in perception. This is what causes sensory hyposensitivities and hypersensitivities. They do not affect only the five main senses—many sensory systems are involved, including the less visible ones I discuss here.
Cognitively, all of this manifests as more analytical, logical, pattern-focused thinking and a strong investment in specific domains—special interests. This is also linked to an imbalance between two neurotransmitters: glutamate (excitatory) and GABA (inhibitory). Concretely, this results in excessive excitation and reduced inhibition (which normally filters information). Levels of serotonin (“happiness” hormone), dopamine (reward hormone), and oxytocin (social bonding hormone) are also subject to atypical regulation in the brain, affecting social relationships and specific interests.
A multifactorial origin
ASD has multiple origins: biological, genetic, and environmental. It is heritable at around 50%. More than 500 genes involved in autism have already been identified. I myself underwent genetic testing to identify genes correlated with my autism, which I will probably discuss in a future article. At least two genes were identified (and yes, that is already meaningful—mathematically, it’s above zero!).
When we speak of environmental factors, this refers to genes interacting with prenatal environmental influences. Pregnancy complications are often—but not systematically—reported, and this question is sometimes asked during the diagnostic process. Autism is therefore not an acquired disease but a neurodevelopmental difference.
Its manifestations
Differences in interaction and communication
Autism is primarily characterized by differences in the nature of verbal and nonverbal communication and in social interaction. This often appears as minimal body language or, conversely, very expressive communication, whether in facial expressions or full-body cues. Prosody (rhythm, tone, intonation) is often more neutral or monotone, or sometimes more melodic. Nonverbal decoding is typically affected.
This skill is not innate but can be learned when an autistic person compensates. I myself reportedly have a fairly monotone voice (with my level of self-analysis, I don’t notice it), but I adapt it depending on my audience. And when my intonation wavers, it’s usually a sign that something is wrong. As for facial expressions, I learned—through hundreds of films—to analyze others’ expressions. It happens in real time.
My psychologist told me it was as if I were in front of a control panel, activating buttons as needed based on what I perceived. It is an ultra-fast process that, yes, makes me highly efficient at reading nonverbal cues. And despite that, I can still be caught off guard by an expression, which tends to leave me very confused.
Autistic people can interact and often seek interaction with others, but they use different social codes that may lead to isolation. This is not universal: some autistic people prefer being alone and self-focused. When that is the case, it should be accepted and the person should not be forced to behave otherwise.
Repetitive patterns
Autism also often manifests as what is perceived as a rigid adherence to routines and rituals, which provide structure to daily life in a world experienced as unpredictable. These repetitive actions are generally soothing, even if they may sometimes appear counterproductive from the outside.
Autistic people also typically have so-called special interests in which they find comfort and safety and in which they may become highly knowledgeable. I describe my own specific interests and their usefulness in more depth in this article.
A large majority of autistic people also engage in stimming—repetitive movements that may resemble tics but actually serve a different function: sensory and emotional self-regulation. This is linked to the sensory hyposensitivities and hypersensitivities discussed earlier in the article. I discuss this more specifically in this article on stims.
Women and autism
Here is some information regarding autism in women, but for a more detailed overview, see the dedicated article featuring testimony from Jeanne, an autistic friend, and her raw, unfiltered lived experience.
A great deal of diagnostic wandering
Women represent about 1 in 4 autistic individuals. This figure may evolve, as it is likely influenced by underdiagnosis. Ten years ago, the number was even lower. Numerous studies suggest that autism in women is widely underdiagnosed or diagnosed late due to criteria based on male stereotypes, possible psychiatric comorbidities, and the factors mentioned above.
One study suggests that the current structure of diagnostic criteria contributes to this widespread bias (MDPI, 2025, ASD in Women). Another study reports that 80% of autistic women remain undiagnosed before age 18 (Nature, 2024).
Many autistic women are also misdiagnosed with other conditions—such as social anxiety or borderline personality disorder—when an autism diagnosis would be more appropriate. These misdiagnoses can create confusion and may even be harmful if managed inappropriately.
Less atypical special interests
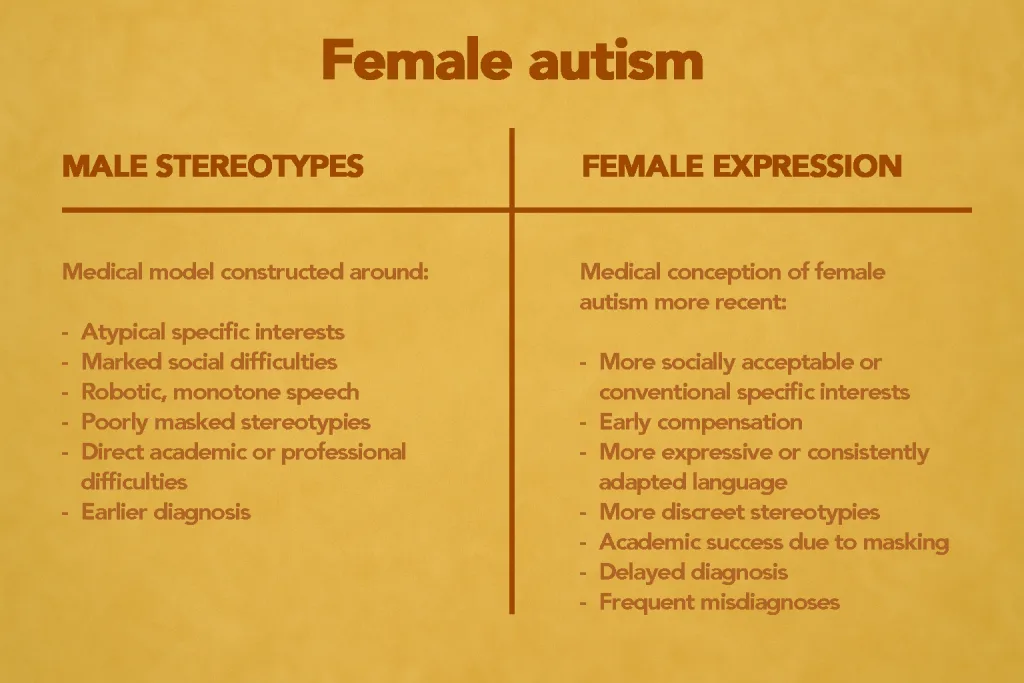
Their special interests are often less atypical and more “socially acceptable.” Yet they may devote just as much intense time to them as men do. It is important to understand that the medical conception of autism was built around male stereotypes.
The ADOS-2, a diagnostic tool very commonly used by professionals, also includes criteria related to special interests. It has been shown that the tool reaches its limits when assessing women. A 2022 study reported that use of the ADOS-2 led to an exclusion rate for women 2.5 times higher than for men (PMC, Exclusion of females in autism research). This is notably explained by their high level of compensation.
Compensatory strategies adopted very early
Autistic women also often adopt compensatory strategies very early to appear typical: observing and imitating others’ behaviors (sometimes even practicing in front of a mirror, according to a concerned friend), and learning relational codes. Society also places different expectations on women than on men: from childhood, girls are expected to be well-behaved, empathetic, and sociable. This pushes many—again—to compensate and mask very early in order to meet these norms.
Autism and its strengths
The DSM tends to speak in terms of deficits (where one might instead speak of differences) in communication and interaction, but autism often comes with unique strengths: specialized thinking styles (visual, logical, pattern-based), exceptional hyperfocus when the person engages in a task, and often remarkable memory. Autistic people are also often less susceptible to certain cognitive biases (such as the framing effect) and may speak their mind more directly. While this can sometimes create difficulties, it can also be a strength. Loyalty, frankness, and honesty are frequently strongly observed in autistic individuals.
Comorbidities
Without transition, comorbidities occupy a major place in autism diagnoses. Put simply, if you think a small portion of the general population shares a given mental condition, multiply that figure to estimate its prevalence in autism. This is a deliberate exaggeration, but it reflects a real trend: autistic people often have additional comorbidities.
ADHD (attention deficit hyperactivity disorder, with or without hyperactivity) is one of the main ones, observed in 50 to 70% of autistic individuals. Epilepsy is also highly represented, affecting about 30% of autistic people.
Schizophrenia also appears more frequently in autism, as does bipolar disorder—type I in my case.
For my part, I am autistic, bipolar, dyspraxic, and have ADHD. Accumulating diagnoses when you are autistic is actually quite common (I even had fun calculating the probability of having all these conditions—it was low).
Key figures
Autism is far more prevalent than one might think. Its prevalence varies by country. This variability is debated and may be explained by a very high rate of underdiagnosis—and possibly some overdiagnosis linked, among other things, to the broadening of DSM-5 diagnostic criteria.
Here are some statistics related to autism:
📊 A highly prevalent condition
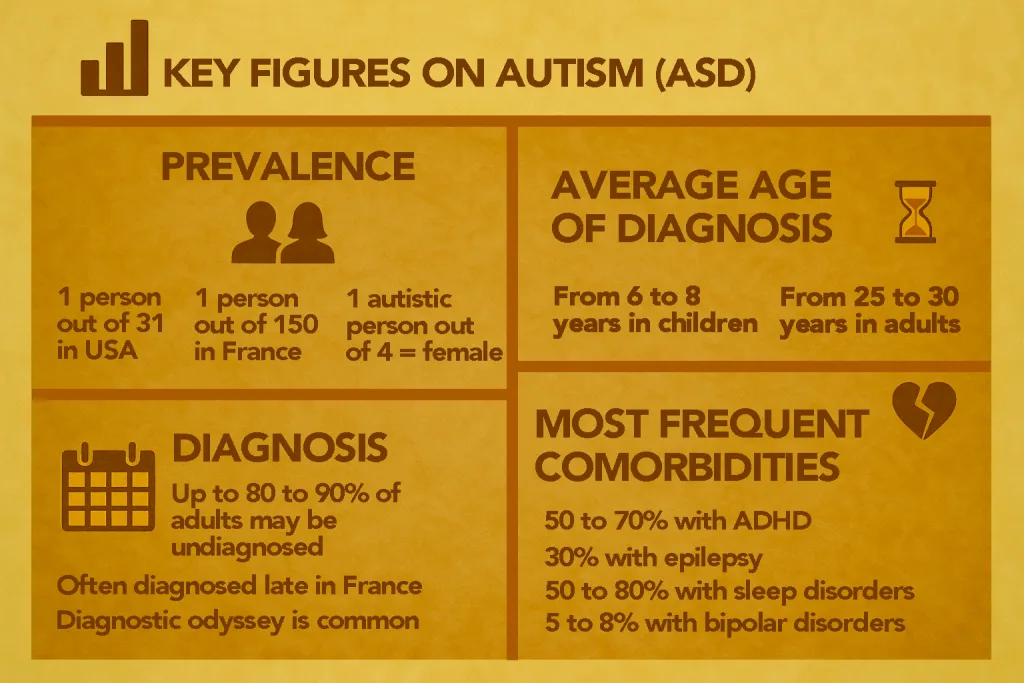
- In France, autism is estimated to affect about 1 in 150 people
- Approximately 700,000 people are estimated to be autistic in France
- Only around 75,000 have received a formal diagnosis
- In the United States, recent estimates suggest a prevalence of about 1 in 31 children
- Roughly 1 in 4 autistic individuals is assigned female at birth (likely an underestimate)
- Global estimates have risen dramatically over time, from about 1 in 5,000 in the 1970s to around 1 in 100 today according to the WHO
- Up to 80–90% of autistic adults may remain undiagnosed
🩺 Table of main comorbidities
According to Autism Spectrum News:
| Comorbidity | Prevalence |
|---|---|
| ADHD | 50 to 70% |
| Epilepsy | 30% |
| Anxiety | 30% |
| Depression | 26% |
| Bipolar disorder | 5 to 8% |
| Schizophrénia | 5 to 7% |
| Sleep disorders | 50 to 80% |
| Gastrointestinal disorders | 46 to 84% |
Here is an interesting interactive map to explore global autism prevalence figures in more detail, based on various studies.
Common misconceptions
“An autistic person doesn’t make eye contact”
Reality: Many autistic people can or have learned, through masking, to make eye contact. (In fact, I’m almost convinced I do… unless I’m actually staring at people’s ears.)
“All autistic people are gifted”
Reality: The IQ distribution is similar to that of the general population (≈ 51–59% ≥ 86 in a large cohort).
“Autistic people don’t want friends”
Reality: Most autistic people seek social interaction but have difficulty forming connections due to implicit social codes.
“Autism is a disease”
Reality: Autism is a neurodevelopmental condition and therefore not something to be cured. We speak of differences rather than deficits.
“You’re a girl, you can’t be autistic”
Reality: Women are simply much more underdiagnosed than men due to masking that is often developed very early.
I invite you to read this article, which debunks the most common myths about autism.
📋 TL;DR: Autism in short
- Spectrum: every autistic person is unique, with varied strengths and vulnerabilities.
- Origin: combination of genetic factors (more than 500 genes involved) and early environmental influences, present from pregnancy.
- Brain: local hyperconnectivity, long-range hypoconnectivity, glutamate/GABA imbalance, atypical regulation of dopamine, serotonin, and oxytocin.
- Manifestations: differences in communication, social interactions, sensory processing, routines, and specific interests.
- Women: often underdiagnosed due to masking and male-based medical stereotypes.
- Comorbidities: ADHD (50–70%), epilepsy (30%), anxiety and depression (≈30%), sleep disorders (50–80%), etc.
- Strengths: hyperfocus, remarkable memory, original thinking (logical, visual, pattern-based), loyalty, and frankness.
- Misconceptions: lack of empathy, absence of social life, rarity in women → all false.
- Key figures: 1 in 31 in the United States, 1 in 100 worldwide, up to 80–90% of adults undiagnosed.
Originally published in French on: 12 Oct 2025 — translated to English on: 27 Feb 2026.