Many autistic people have experienced — or will experience — at least one autistic burnout in their lifetime. For many, it becomes a diagnostic turning point. Professionals, often poorly informed on the subject, frequently misdiagnose it as depression. To their credit, the phenomenon is widely known within the community but still remains poorly explored in the scientific literature. Yet autistic burnout is a very different syndrome from depression.
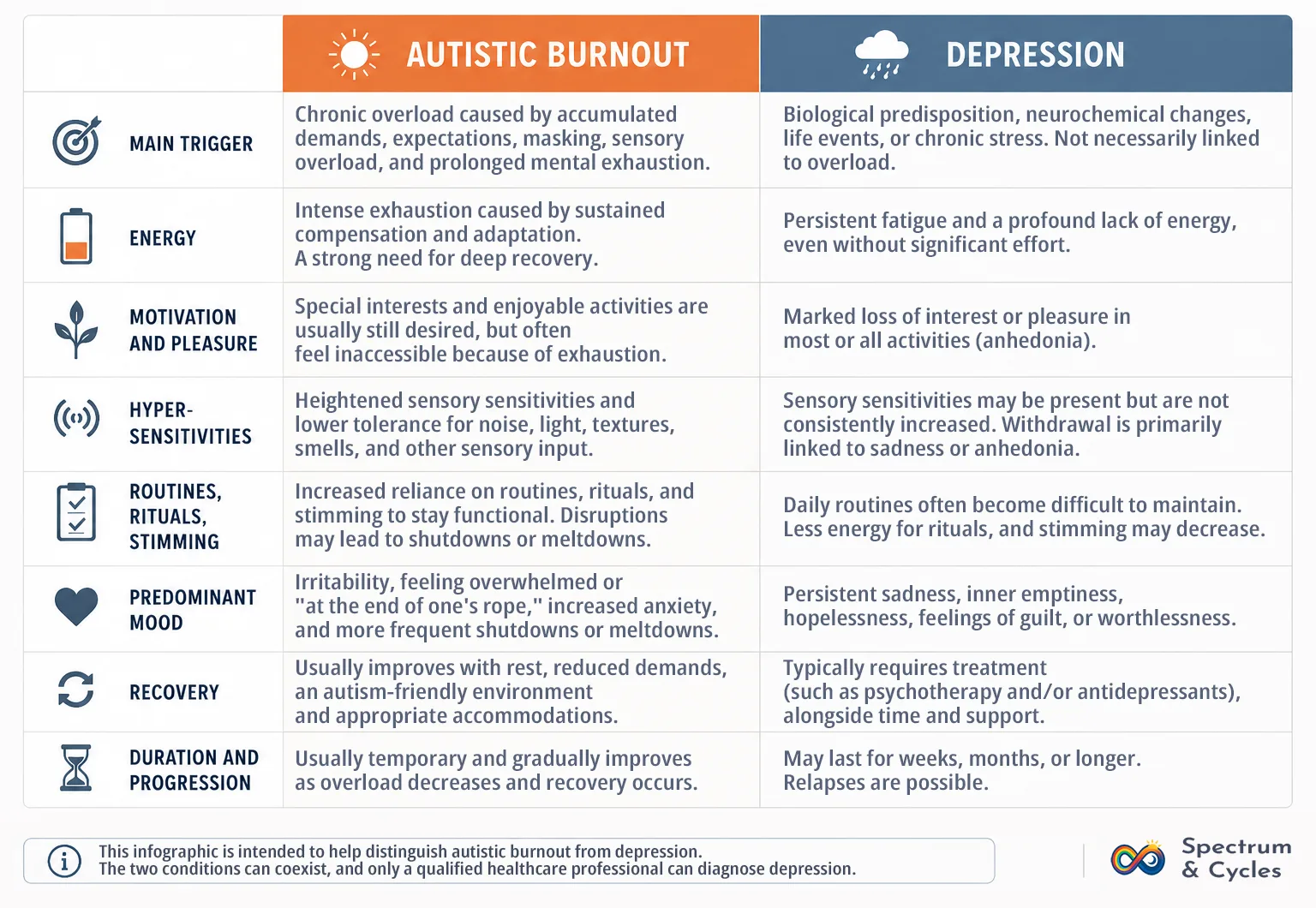
So why does this confusion exist, and why is it so common? The difference between autistic burnout and depression mainly lies in the origin of the symptoms, motivation, and the response to overload.
In Brief:
- Cause: autistic burnout is a response to prolonged overload, whereas depression is primarily a mood disorder.
- Shared symptoms: both can involve extreme fatigue, social withdrawal, and major difficulties with daily functioning.
- Key difference: motivation often remains intact in autistic burnout but typically collapses during depression.
- Key point: how your symptoms respond to a calm, autism-friendly environment is often one of the clearest ways to tell them apart.
Sometimes, even among my autistic friends, I notice confusion between autistic burnout and depression. In fact, one can sometimes lead to the other, and vice versa, making the nature of the person’s suffering difficult to identify. For people with chronic depression or bipolar disorder (like me), the distinction becomes even more complicated.
The psychiatrists who followed me appreciated how deeply I understood myself and my own functioning, yet I was initially identified as depressed before eventually being referred to my specialist center (where my autism assessment took place). It was there that the depressive hypothesis was ruled out, and my psychiatrist first spoke to me about autistic burnout.
Overlapping symptoms
Depression, especially in autistic people, can manifest through symptoms that are relatively similar.
Extreme fatigue
In both cases, the person may spend far more time sleeping without ever feeling rested. Nevertheless, autistic burnout often involves a much deeper level of exhaustion than depression.
In depression
In depression, people often struggle to get out of bed because of fatigue, but above all because of a loss of motivation and ability to do so, caused by the depressive mood itself (typically expressed through profound sadness or severe anxiety).
In autistic burnout
In autistic burnout, a person may sleep through most of the day and still wake up completely exhausted. The body and brain simply do not recover. This is due to the nature of the fatigue itself: it is cognitive, social, sensory, emotional, and even physical. In short, every sphere of the autistic person’s life is affected by autistic burnout.
Altered sensory sensitivities
I do not personally experience this, but autistic people may notice changes in their sensory sensitivities during depression, mainly through more subtle hypersensitivities. In my case, they become numbed.
However, it is especially during autistic burnout that affected individuals can experience such an amplification of sensory hypersensitivities that they sometimes become unable to leave their homes.
- Sunlight (even during cloudy weather) can become unbearable
- Environmental noises outside may become extremely difficult to handle
- Taste sensitivities may intensify to the point where meals are no longer varied and previously enjoyable foods lose all appeal
- Smells can become invasive and prevent going outside
- Even the slightest tactile contact may become unbearable
The entire sensory system is affected. In my own case, the most intriguing change was the transition from olfactory hyposensitivity (I could barely smell anything) to a hypersensitivity that kept intensifying over time. It remained hypersensitive even after the burnout had ended.
Intensification of autistic traits
Autistic burnout
Alongside heightened sensory sensitivities, stimming naturally becomes much more frequent for many autistic people. Some even develop new stims and may therefore appear “more autistic,” whereas depression often makes them seem more inert or withdrawn. Attachment to rituals and routines also becomes much stronger, as does rigidity. This is largely caused by the overall overload experienced by the autistic person — something that is not at the core of depression.
Depression
By contrast, during depression, energy collapses and the difficulty of maintaining everyday life often reduces these autistic traits. Routines usually help bring structure to the lives of autistic people, and they therefore often disappear during depression. However, this is not systematic: some autistic people maintain their rituals or stims, but these are not behaviors caused by depression itself. They may instead be responses to a concurrent autistic burnout.
Anhedonia
The main symptom of depression is anhedonia: the loss of desire or pleasure in activities that are normally enjoyable. In short, motivation collapses. This is especially visible in autistic people, who often devote a large portion of their time to their special interests.
When I am in the middle of a depressive episode, I stop watching movies, I stop coding, and I stop reading: I stop doing anything at all. And this is extremely destabilizing, which is why I felt so confused during the years preceding my autism and bipolar disorder diagnoses.
This is something rarely observed in autistic burnout. And when a reduction in activity does appear, it is generally linked to exhaustion rather than loss of interest. Motivation remains intact and the desire to engage is still present, which distinguishes it from depression — and is my main criterion for telling the two apart.
Links with overload
Virtually all behaviors associated with autistic burnout are connected in one way or another to overload. As a result, autistic crises often become more frequent and social isolation more pronounced. It is an automatic response from the brain — a survival mode activated until the overload decreases and the autistic person can rest and return to a more suitable environment.
The same applies to executive functioning, which can become severely impaired during autistic burnout. In depression, however, these difficulties are more often linked to psychomotor slowing and lack of energy.
Mood-related issues
There are also major differences between autistic burnout and depression when it comes to mood. Depressive mood (sadness/anxiety), low self-worth, and suicidal thoughts are typical features of depression, but are usually far less present in autistic burnout.
Improvement of the condition
One important question to ask yourself is: “What happens to my condition when I am in a calm, safe environment adapted to my needs?”
- “My condition improves, I feel less exhausted” → Autistic burnout: the syndrome tends to stabilize as sensory and social overload decreases.
- “My condition does not improve” → Depression: depression is more constant and can worsen over time independently of environmental factors such as sensory overload.
In fact, depression persists even in the absence of overload (even if its intensity naturally fluctuates throughout the day).
Onset / recovery
Depression often develops gradually, or abruptly in bipolar people at the end of a (hypo)manic episode. In bipolar disorder, this is thought to result from severe neurotransmitter depletion, leading to what many describe as a “crash” (mood suddenly collapses after an intense elevation).
Autistic burnout, on the other hand, is usually much more abrupt (regardless of whether the person is bipolar or not), similarly to an autistic crisis such as a shutdown or meltdown. It gradually fades as overload becomes regulated and the autistic person gains a better understanding of their own needs.
Even though it can appear suddenly, autistic burnout often comes with early warning signs that can be noticed beforehand.
Depression also eventually comes to an end over time, but it usually requires medical treatment prescribed by a psychiatrist, often involving antidepressants or mood stabilizers in bipolar individuals. The reason is that depression involves complex biological and neurochemical mechanisms, which explains why medical treatment is often necessary.
Autistic burnout, on the other hand, is a neurological response to overload for which no direct treatment exists. It is a signal that the person needs to stop and rethink their daily life.
Do you think you may be experiencing autistic burnout? I’ve written a detailed guide on recovery strategies, environmental adaptations, and ways to prevent relapse.
The difficulty of distinguishing the two
Considering all these factors, it becomes easier to understand why distinguishing autistic burnout from depression can be so difficult, even though the symptoms differ in important ways. Research still needs to progress on the subject, and the medical field needs greater awareness of it. Diagnostic wandering can be extremely confusing, and the near-systematic prescription of treatments for the wrong diagnosis can be deeply problematic for the people concerned.
Better understanding these signs — and better understanding oneself — often helps people move forward more quickly with professionals. What matters most is maintaining clear and precise communication with healthcare providers. It would be dangerous to medically treat an autistic burnout, but also dangerous not to treat a depression mistakenly assumed to be burnout.
